Bursitis Ball Of Foot Treatment Method
Overview
Retrocalcaneal bursitis is the painful inflammation and swelling of the retrocalcaneal bursa that is situated between the calcaneus (heel bone) and the Achilles tendon. A bursa is a small fluid filled sac that forms around joints in areas where there is a lot of friction between muscles, tendons and outcrops of bone. The bursae position themselves in between the tendon or muscle and the bone, buffering any friction from movement. To picture a bursa imagine it as a very small water filled balloon that sits in places where things rub against each other, such as in between a tendon and a bone, to provide a soft smooth cushion for the tendon to pass over painlessly. The covering of the bursa also acts as a lubricant and aids the tendon?s movement. It is estimated that there is over 150 bursae in your body which protect the joint and tendons from wear. They are all very small and unnoticeable until they become swollen and painful with bursitis.
Causes
Age. Bursitis is more common during middle age due to repetitive activities that put wear and tear on the body over time. Certain activities or occupations. If your job or hobby involves repetitive motion or puts pressure on bursae, you have a higher likelihood of developing bursitis. Reaching overhead, leaning elbows on arm rests, crossing your legs, laying carpet, setting tile, gardening, biking, playing baseball and ice skating are some activities that, when repeated very often, can put you at increased risk of developing bursitis. Sports in which you may get hit in the knee or fall to the knees, such as football, can also increase the risk. Some medical or health conditions. Rheumatoid arthritis, osteoarthritis, gout, thyroid disease, diabetes, alcoholism and some immunosuppressive disorders can increase the risk of bursitis. The reasons can vary, from cartilage breakdown around joints (arthritis) to crystals in the bursa that cause inflammation (gout). Wearing high heels. Posterior Achilles tendon bursitis occurs when the bursa located between the skin and the Achilles tendon (the band of tissue that attaches the calf muscle to the heel bone) becomes inflamed. High heels are often to blame for this, the stiff heel can put direct pressure on the bursa between the skin and the Achilles tendon.
Symptoms
Unlike Achilles tendinitis, which tends to manifest itself slightly higher on the lower leg, Achilles tendon bursitis usually creates pain and irritation at the back of the heel. Possible signs of bursitis of the Achilles tendon include difficulty to rise on toes. Standing on your toes or wearing high heels may increase the heel pain. Inflammation and tenderness. The skin around your heel can become swollen and warm to the touch. Redness may be visible. Pain in the heel. Pain tends to become more prominent when walking, running, or touching the inflamed area. Stiffness. The back of your ankle may feel a little stiff due to the swelling of the bursa.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
Your health care provider may recommend the following treatments. Avoid activities that cause pain. Ice the heel several times a day. Take nonsteroidal anti-inflammatory medications (for example, ibuprofen). Try over-the-counter or custom heel wedges to help decrease the stress on the heel. Try ultrasound treatment during physical therapy to reduce inflammation. Use physical therapy to improve flexibility and strength around the ankle, which can help the bursitis improve and prevent it from coming back. If these treatments don't work, your health care provider may inject a small amount of steroids into the bursa. After the injection, you should avoid stretching the tendon too much because it can break open (rupture). If the condition is connected with Achilles tendinitis, casting the ankle for several weeks to keep it from moving can be effective. Very rarely, surgery may be needed to remove the inflamed bursa.
Surgical Treatment
Surgery to remove the damaged bursa may be performed in extreme cases. If the bursitis is caused by an infection, then additional treatment is needed. Septic bursitis is caused by the presence of a pus-forming organism, usually staphylococcus aureus. This is confirmed by examining a sample of the fluid in the bursa and requires treatment with antibiotics taken by mouth, injected into a muscle or into a vein (intravenously). The bursa will also need to be drained by needle two or three times over the first week of treatment. When a patient has such a serious infection, there may be underlying causes. There could be undiscovered diabetes, or an inefficient immune system caused by human immunodeficiency virus infection (HIV).
Retrocalcaneal bursitis is the painful inflammation and swelling of the retrocalcaneal bursa that is situated between the calcaneus (heel bone) and the Achilles tendon. A bursa is a small fluid filled sac that forms around joints in areas where there is a lot of friction between muscles, tendons and outcrops of bone. The bursae position themselves in between the tendon or muscle and the bone, buffering any friction from movement. To picture a bursa imagine it as a very small water filled balloon that sits in places where things rub against each other, such as in between a tendon and a bone, to provide a soft smooth cushion for the tendon to pass over painlessly. The covering of the bursa also acts as a lubricant and aids the tendon?s movement. It is estimated that there is over 150 bursae in your body which protect the joint and tendons from wear. They are all very small and unnoticeable until they become swollen and painful with bursitis.
Causes
Age. Bursitis is more common during middle age due to repetitive activities that put wear and tear on the body over time. Certain activities or occupations. If your job or hobby involves repetitive motion or puts pressure on bursae, you have a higher likelihood of developing bursitis. Reaching overhead, leaning elbows on arm rests, crossing your legs, laying carpet, setting tile, gardening, biking, playing baseball and ice skating are some activities that, when repeated very often, can put you at increased risk of developing bursitis. Sports in which you may get hit in the knee or fall to the knees, such as football, can also increase the risk. Some medical or health conditions. Rheumatoid arthritis, osteoarthritis, gout, thyroid disease, diabetes, alcoholism and some immunosuppressive disorders can increase the risk of bursitis. The reasons can vary, from cartilage breakdown around joints (arthritis) to crystals in the bursa that cause inflammation (gout). Wearing high heels. Posterior Achilles tendon bursitis occurs when the bursa located between the skin and the Achilles tendon (the band of tissue that attaches the calf muscle to the heel bone) becomes inflamed. High heels are often to blame for this, the stiff heel can put direct pressure on the bursa between the skin and the Achilles tendon.
Symptoms
Unlike Achilles tendinitis, which tends to manifest itself slightly higher on the lower leg, Achilles tendon bursitis usually creates pain and irritation at the back of the heel. Possible signs of bursitis of the Achilles tendon include difficulty to rise on toes. Standing on your toes or wearing high heels may increase the heel pain. Inflammation and tenderness. The skin around your heel can become swollen and warm to the touch. Redness may be visible. Pain in the heel. Pain tends to become more prominent when walking, running, or touching the inflamed area. Stiffness. The back of your ankle may feel a little stiff due to the swelling of the bursa.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
Your health care provider may recommend the following treatments. Avoid activities that cause pain. Ice the heel several times a day. Take nonsteroidal anti-inflammatory medications (for example, ibuprofen). Try over-the-counter or custom heel wedges to help decrease the stress on the heel. Try ultrasound treatment during physical therapy to reduce inflammation. Use physical therapy to improve flexibility and strength around the ankle, which can help the bursitis improve and prevent it from coming back. If these treatments don't work, your health care provider may inject a small amount of steroids into the bursa. After the injection, you should avoid stretching the tendon too much because it can break open (rupture). If the condition is connected with Achilles tendinitis, casting the ankle for several weeks to keep it from moving can be effective. Very rarely, surgery may be needed to remove the inflamed bursa.
Surgical Treatment
Surgery to remove the damaged bursa may be performed in extreme cases. If the bursitis is caused by an infection, then additional treatment is needed. Septic bursitis is caused by the presence of a pus-forming organism, usually staphylococcus aureus. This is confirmed by examining a sample of the fluid in the bursa and requires treatment with antibiotics taken by mouth, injected into a muscle or into a vein (intravenously). The bursa will also need to be drained by needle two or three times over the first week of treatment. When a patient has such a serious infection, there may be underlying causes. There could be undiscovered diabetes, or an inefficient immune system caused by human immunodeficiency virus infection (HIV).
How To Help Hammertoe Pain
 Overview
Overview
A Hammer toes occurs from a muscle and ligament imbalance around the toe joint which causes the middle joint of the toe to bend and become stuck in this position. The most common complaint with hammertoes is rubbing and irritation on the top of the bent toe. Toes that may curl rather than buckle, most commonly the baby toe, are also considered hammertoes. It can happen to any toe. Women are more likely to get pain associated with hammertoes than men because of shoe gear. Hammertoes can be a serious problem in people with diabetes or poor circulation. People with these conditions should see a doctor at the first sign of foot trouble.
Causes
Medical problems, such as stroke or diabetes that affect the nerves, may also lead to hammertoe. For example, diabetes can result in poor circulation, especially in the feet. As a result, the person may not feel that their toes are bent into unnatural positions. The likelihood of developing hammertoe increases with age and may be affected by gender (more common in women) and toe length; for example, when the second toe is longer than the big toe, hammertoe is more likely to occur. Hammertoe may also be present at birth. Genetics may factor in to developing hammertoe, particularly if the foot is flat or has a high arch, resulting in instability.
 Symptoms
Symptoms
The most obvious sign of hammertoes are bent toes, other symptoms may include pain and stiffness during movement of the toe. Painful corns on the tops of the toe or toes from rubbing against the top of the shoe's toe box. Painful calluses on the bottoms of the toe or toes. Pain on the bottom of the ball of the foot. Redness and swelling at the joints.
Diagnosis
Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look Hammer toes for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. If the deformed toe is very painful, your doctor may recommend that you have a fluid sample withdrawn from the joint with a needle so the fluid can be checked for signs of infection or gout (arthritis from crystal deposits).
Non Surgical Treatment
Apply a commercial, nonmedicated hammertoe pad around the bony prominence of the hammertoe. This will decrease pressure on the area. Wear a shoe with a deep toe box. If the hammertoe becomes inflamed and painful, apply ice packs several times a day to reduce swelling. Avoid heels more than two inches tall. A loose-fitting pair of shoes can also help protect the foot while reducing pressure on the affected toe, making walking a little easier until a visit to your podiatrist can be arranged. It is important to remember that, while this treatment will make the hammertoe feel better, it does not cure the condition. A trip to the podiatric physician?s office will be necessary to repair the toe to allow for normal foot function. Avoid wearing shoes that are too tight or narrow. Children should have their shoes properly fitted on a regular basis, as their feet can often outgrow their shoes rapidly. See your podiatric physician if pain persists.
Surgical Treatment
If you have a severe case of hammer toe or if the affected toe is no longer flexible, you may need surgery to straighten your toe joint. Surgery requires only a local anesthetic (numbing medicine for the affected area) and is usually an outpatient procedure. This means you don?t have to stay in the hospital for the surgery.
What Are Bunions?
Overview
 When the big toe is misaligned, it creates an unnatural bump on the inside of the forefoot (see image below). In addition to being unsightly, the lump or bunion can cause pain and make buying shoes difficult. Some people are born predisposed to bunions. But most people acquire them over time from ill-fitting footwear that squeezes the big toe inward toward the other toes. About four out of five bunion pain patients are female, a near perfect fit for the bad shoe theory. The good news, Bunions can be corrected, often with better-fitting shoes and custom orthotics. There are also some cases that cause severe bunion pain and do not respond to conservative treatment. For those patients, bunion surgery called bunionectomy may be necessary.
When the big toe is misaligned, it creates an unnatural bump on the inside of the forefoot (see image below). In addition to being unsightly, the lump or bunion can cause pain and make buying shoes difficult. Some people are born predisposed to bunions. But most people acquire them over time from ill-fitting footwear that squeezes the big toe inward toward the other toes. About four out of five bunion pain patients are female, a near perfect fit for the bad shoe theory. The good news, Bunions can be corrected, often with better-fitting shoes and custom orthotics. There are also some cases that cause severe bunion pain and do not respond to conservative treatment. For those patients, bunion surgery called bunionectomy may be necessary.
Causes
Bunions are a result of complex biomechanical changes that occur in your feet. The type of footwear that you wear does cause bunions. We know that foot bunions occur in about 30% of the population of most Western countries but only 3% in Eastern countries. They are seen most commonly in women and become more common as people get older. Tight-fitting shoes are thought to be the main cause of bunions.. Shoes such as high heels and shoes with tight toe boxes (eg womens fashion shoes and cowboy boots) are particularly damaging to the toes. These shoes have a sloping foot bed and a narrow toe box. The slope causes the front of the foot to bear your weight, which encourages your forefoot to widen. Also, the angle pushes your toes into the narrow toe box, causing the toes to become angled and squeezed together.
Symptoms
Many people with bunions suffer from discomfort and pain from the constant irritation, rubbing, and friction of the enlargement against shoes. The skin over the toe becomes red and tender. Because this joint flexes with every step, the bigger the bunion gets, the more it hurts to walk. Over time, bursitis or arthritis may set in, the skin on the bottom of the foot may become thicker, and everyday walking may become difficult-all contributing to chronic bunion pain.
Diagnosis
Looking at the problem area on the foot is the best way to discover a bunion. If it has the shape characteristic of a bunion, this is the first hint of a problem. The doctor may also look at the shape of your leg, ankle, and foot while you are standing, and check the range of motion of your toe and joints by asking you to move your toes in different directions A closer examination with weight-bearing X-rays helps your doctor examine the actual bone structure at the joint and see how severe the problem is. A doctor may ask about the types of shoes you wear, sports or activities (e.g., ballet) you participate in, and whether or not you have had a recent injury. This information will help determine your treatment.
Non Surgical Treatment
Bunion pain can be successfully managed in the vast majority of cases by switching to shoes that fit properly and don't compress the toes. Your orthopaedic surgeon can give you more information about proper shoe fit and the types of shoes that would be best for you. Follow these general points of shoe fit. Do not select shoes by the size marked inside the shoe. Sizes vary among shoe brands and styles. Judge the shoe by how it fits on your foot. Select a shoe that conforms as nearly as possible to the shape of your foot. Have your feet measured regularly. The size of your feet change as you grow older. Have both feet measured. Most people have one foot larger than the other. Fit to the largest foot. Fit at the end of the day when your feet are the largest. Stand during the fitting process and check that there is adequate space (3/8" to 1/2") for your longest toe at the end of each shoe. Make sure the ball of your foot fits well into the widest part (ball pocket) of the shoe. Do not purchase shoes that feel too tight, expecting them to "stretch" to fit. Your heel should fit comfortably in the shoe with a minimum amount of slippage. Walk in the shoe to make sure it fits and feels right. (Fashionable shoes can be comfortable.) Some shoes can be modified by stretching the areas that put pressure on your toes. Splints to reposition the big toe and orthotics (special shoe inserts shaped to your feet) also may relieve pain. For bunions caused by arthritis, medications can be prescribed to reduce pain and swelling. 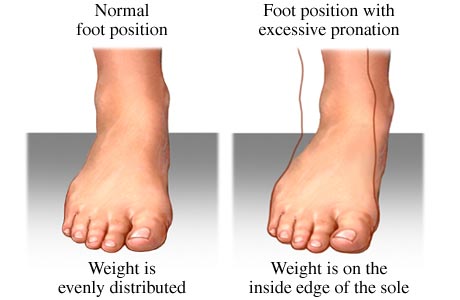
Surgical Treatment
Most bunions can be treated without surgery. But when nonsurgical treatments are not enough, surgery can relieve your pain, correct any related foot deformity, and help you resume your normal activities. An orthopaedic surgeon can help you decide if surgery is the best option for you. Whether you?ve just begun exploring treatment for bunions or have already decided with your orthopaedic surgeon to have surgery, this booklet will help you understand more about this valuable procedure.
Prevention
To help prevent bunions, select your style and size of shoes wisely. Choose shoes with a wide toe area and a half-inch of space between the tip of your longest toe and the end of the shoe. Shoes also should conform to the shape of your feet without causing too much pressure.
Over-Pronation Of The Foot What Are The Causes
Overview
Pronation is the term used to describe a natural movement of the foot when walking. When the gait is normal, the heel strikes the ground first. As weight is transferred forward, the arch of the foot flattens and the foot rolls slightly inwards. Body weight is then placed on the ball of the foot and toes, and the foot straightens and turns outwards as the toes push off. Overpronation occurs when the foot rolls inward too far. This causes all the muscles and tendons of the lower leg to twist excessively. Regular overpronation is believed to contribute to the development of many knee, lower leg and foot injuries such as heel spurs, plantar fasciitis, tendinitis and bunions. It is thought that as much as 60% of the population may overpronate.
Causes
For those not familiar with the term pronation, you might be familiar with terms related to shoes and pronation such as ?motion control?, ?stability,? and ?neutral cushioned.? The terms motion control and stability are typically associated with the word ?over-pronation? or a foot that is supposedly pronating too much and needs correction. According to the running shoe industry, ?over-pronation? is a biomechanical affliction evident when the foot and or ankle rolls inward past the vertical line created by your leg when standing.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis. Achilles tendonopathy. Hallus Valgus and/or bunions. Patellofemoral pain syndrome. Iliotibial band pain syndrome. Low back pain. Shin splints. Stress fractures in the foot or lower leg.
Diagnosis
So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot.
Non Surgical Treatment
An orthotic is a device inserted inside the shoe to assist in prevention and/or rehabilitation of injury. Orthotics support the arch, prevent or correct functional deformities, and improve biomechanics. Prescription foot orthoses are foot orthoses which are fabricated utilizing a three dimensional representation of the plantar foot and are specifically constructed for an individual using both weightbearing and nonweightbearing measurement parameters and using the observation of the foot and lower extremity functioning during weightbearing activities. Non-prescription foot orthoses are foot which are fabricated in average sizes and shapes in an attempt to match the most prevalent sizes and shapes of feet within the population without utilizing a three dimensional representation of the plantar foot of the individual receiving the orthosis.
Prevention
With every step we take, we place at least half of our body weight on each foot (as we walk faster, or run, we can exert more than twice our body weight on each foot). As this amount of weight is applied to each foot there is a significant shock passed on to our body. Custom-made orthotics will absorb some of this shock, helping to protect our feet, ankles, knees, hips, and lower back.
Pronation is the term used to describe a natural movement of the foot when walking. When the gait is normal, the heel strikes the ground first. As weight is transferred forward, the arch of the foot flattens and the foot rolls slightly inwards. Body weight is then placed on the ball of the foot and toes, and the foot straightens and turns outwards as the toes push off. Overpronation occurs when the foot rolls inward too far. This causes all the muscles and tendons of the lower leg to twist excessively. Regular overpronation is believed to contribute to the development of many knee, lower leg and foot injuries such as heel spurs, plantar fasciitis, tendinitis and bunions. It is thought that as much as 60% of the population may overpronate.
Causes
For those not familiar with the term pronation, you might be familiar with terms related to shoes and pronation such as ?motion control?, ?stability,? and ?neutral cushioned.? The terms motion control and stability are typically associated with the word ?over-pronation? or a foot that is supposedly pronating too much and needs correction. According to the running shoe industry, ?over-pronation? is a biomechanical affliction evident when the foot and or ankle rolls inward past the vertical line created by your leg when standing.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis. Achilles tendonopathy. Hallus Valgus and/or bunions. Patellofemoral pain syndrome. Iliotibial band pain syndrome. Low back pain. Shin splints. Stress fractures in the foot or lower leg.
Diagnosis
So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot.
Non Surgical Treatment
An orthotic is a device inserted inside the shoe to assist in prevention and/or rehabilitation of injury. Orthotics support the arch, prevent or correct functional deformities, and improve biomechanics. Prescription foot orthoses are foot orthoses which are fabricated utilizing a three dimensional representation of the plantar foot and are specifically constructed for an individual using both weightbearing and nonweightbearing measurement parameters and using the observation of the foot and lower extremity functioning during weightbearing activities. Non-prescription foot orthoses are foot which are fabricated in average sizes and shapes in an attempt to match the most prevalent sizes and shapes of feet within the population without utilizing a three dimensional representation of the plantar foot of the individual receiving the orthosis.
Prevention
With every step we take, we place at least half of our body weight on each foot (as we walk faster, or run, we can exert more than twice our body weight on each foot). As this amount of weight is applied to each foot there is a significant shock passed on to our body. Custom-made orthotics will absorb some of this shock, helping to protect our feet, ankles, knees, hips, and lower back.
Can One Address Calcaneal Apophysitis In The Home?
Overview
Sever's disease is a painful irritation in the heel bone of the foot. It is the most common cause of heel pain in children and teens. Sever?s disease is also called calcaneal apophysitis.
Causes
Apart from the age of the young person, other factors that may contribute to developing the disease may include; overuse or too much physical activity. Your child?s heel pain may be caused by repeated stress on the heels (running and jumping activities), pressure on the back of the heel from too much standing or wearing poor-fitting shoes. This includes shoes that do not support or provide enough padding for your child?s feet.
Symptoms
The most prominent symptom of Sever's disease is heel pain which is usually aggravated by physical activity such as walking, running or jumping. The pain is localised to the posterior and plantar side of the heel over the calcaneal apophysis. Sometimes, the pain may be so severe that it may cause limping and interfere with physical performance in sports. External appearance of the heel is almost always normal, and signs of local disease such as edema, erythema (redness) are absent. The main diagnostic tool is pain on medial- lateral compression of the calcaneus in the area of growth plate, so called squeeze test. Foot radiographs are usually normal. Therefore the diagnosis of Sever's disease is primarily clinical.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
Treatment may consist of one or more of the following. Elevating the heel. Stretching hamstring and calf muscles 2-3 times daily. Using R.I.C.E. (Rest, Ice, Compression, Elevation). Foot orthotics. Medication. Physical therapy. Icing daily (morning). Heating therapy. Open back shoe are best and avoid high heel shoe. The Strickland Protocol has shown a positive response in patients with a mean return to sport in less than 3 weeks. Further research into the anatomical and biomechanical responses of this protocol are currently being undertaken.
Prevention
Sever?s disease may be prevented by maintaining good flexibility while your child is growing. The stretching exercises mentioned here can lower your child?s risk for injuries during the growth spurt. Good-quality shoes with firm support and a shock-absorbent sole will help. Your child should avoid excessive running on hard surfaces. If your child has already recovered from Sever?s disease, stretching and putting ice on the heel after activity will help keep your child from getting this condition again.
Sever's disease is a painful irritation in the heel bone of the foot. It is the most common cause of heel pain in children and teens. Sever?s disease is also called calcaneal apophysitis.
Causes
Apart from the age of the young person, other factors that may contribute to developing the disease may include; overuse or too much physical activity. Your child?s heel pain may be caused by repeated stress on the heels (running and jumping activities), pressure on the back of the heel from too much standing or wearing poor-fitting shoes. This includes shoes that do not support or provide enough padding for your child?s feet.
Symptoms
The most prominent symptom of Sever's disease is heel pain which is usually aggravated by physical activity such as walking, running or jumping. The pain is localised to the posterior and plantar side of the heel over the calcaneal apophysis. Sometimes, the pain may be so severe that it may cause limping and interfere with physical performance in sports. External appearance of the heel is almost always normal, and signs of local disease such as edema, erythema (redness) are absent. The main diagnostic tool is pain on medial- lateral compression of the calcaneus in the area of growth plate, so called squeeze test. Foot radiographs are usually normal. Therefore the diagnosis of Sever's disease is primarily clinical.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
Treatment may consist of one or more of the following. Elevating the heel. Stretching hamstring and calf muscles 2-3 times daily. Using R.I.C.E. (Rest, Ice, Compression, Elevation). Foot orthotics. Medication. Physical therapy. Icing daily (morning). Heating therapy. Open back shoe are best and avoid high heel shoe. The Strickland Protocol has shown a positive response in patients with a mean return to sport in less than 3 weeks. Further research into the anatomical and biomechanical responses of this protocol are currently being undertaken.
Prevention
Sever?s disease may be prevented by maintaining good flexibility while your child is growing. The stretching exercises mentioned here can lower your child?s risk for injuries during the growth spurt. Good-quality shoes with firm support and a shock-absorbent sole will help. Your child should avoid excessive running on hard surfaces. If your child has already recovered from Sever?s disease, stretching and putting ice on the heel after activity will help keep your child from getting this condition again.
Pain In The Arch Of My Foot While Running
Overview
Many people have pain in the base of their foot. This could be due to overuse of one of many different structures in your foot. Common examples are sesamoiditis (inflammation of structures surrounding two small bones under the big toe joint) and plantar fasciitis (overuse of a ligament-like structure that runs underneath the length of the foot). Pain on standing first thing in the morning is a classic symptom of plantar fasciitis. It is one of the most common problems experienced by runners, accounting for about 10 per cent of running injuries. It is also common among middle-aged people, particularly if they are overweight. It often starts with low-grade pain in the arch or heel of the foot and can get worse over weeks or months.

Causes
A common cause of foot arch pain is a stress fracture. They tend to occur from repeated overloading of one of the foot bones from activities such as jumping and running especially if you have suddenly increased your activity level. The breaks in the bone may be small but they can be extremely painful. Stress fractures of the metatarsal bones or the navicular can cause anything from mild to severe foot arch pain. The Tibialis Posterior muscle plays a very important role in supporting the medial arch of the foot. Posterior Tibial Tendonitis can occur either through repetitive use e.g. high impact sports such as soccer or tennis, or from an injury e.g. a fall. This causes the tendon to become inflamed or even torn, resulting in pain on bottom of foot. This pain usually gets worse with activity or when standing for long periods. If the problem persists, the inner side of the foot (known as the medial longitudinal arch of the foot) gradually collapses down, causing flat feet. A simple test for this condition is to stand on one leg and rise up onto your tiptoes. If you cannot, it indicates a problem with the Posterior Tibial tendon. Treatment usually consists of rest, ice, exercises, orthotics and physical therapy.
Symptoms
The majority of children and adults with flexible flatfeet never have symptoms. However, their toes may tend to point outward as they walk, a condition called out-toeing. A person who develops symptoms usually complains of tired, aching feet, especially after prolonged standing or walking. Symptoms of rigid flatfoot vary depending on the cause of the foot problem.
Diagnosis
A professional therapist may use tinels test to diagnose tarsal tunnel syndrome. This involves tapping the nerve just behind the medial malleolus or bony bit of the ankle with a rubber hammer. Pain indicates a positive test. Sometimes it is initially mistaken for plantar fasciitis which also causes pain from the inside heel and throughout the arch of the foot. Neural symptoms (such as tingling or numbness) as well as the location of tenderness when touching the area should help to easily distinguish between the conditions.
Non Surgical Treatment
A new ankle foot orthosis known as the Richie Brace, offered by PAL Health Systems, has proven to show significant success in treating Stage II posterior tibial dysfunction and the adult acquired flatfoot. This is a sport-style brace connected to a custom corrected foot orthotic device that fits well into most forms of lace-up footwear, including athletic shoes. The brace is light weight and far more cosmetically appealing than the traditional ankle foot orthosis previously prescribed.

Surgical Treatment
If you have pain that has not been responsive to other treatments, there is a new non-surgical treatment that was recently approved by the FDA. ESWT (extracorporeal shockwave therapy) uses strong electrohydraulic acoustic (sound) energy that triggers the body?s natural repair mechanism. This treatment method is safe, effective and requires a very short recovery period compared to older surgical techniques.
Prevention
Stretch and strengthen important muscles in your feet, ankles and legs in order to guard against future strain. Make sure to acquire suitable arch supports and inserts if necessary, and that your shoes are shock absorbent and in good condition. Wearing tattered shoes provides no protection, and runners should replace their footwear before exceeding 500 miles of usage. Athletes new to arch supports should gradually build their training routine, allowing their feet to become accustomed to a new stance.
Many people have pain in the base of their foot. This could be due to overuse of one of many different structures in your foot. Common examples are sesamoiditis (inflammation of structures surrounding two small bones under the big toe joint) and plantar fasciitis (overuse of a ligament-like structure that runs underneath the length of the foot). Pain on standing first thing in the morning is a classic symptom of plantar fasciitis. It is one of the most common problems experienced by runners, accounting for about 10 per cent of running injuries. It is also common among middle-aged people, particularly if they are overweight. It often starts with low-grade pain in the arch or heel of the foot and can get worse over weeks or months.
Causes
A common cause of foot arch pain is a stress fracture. They tend to occur from repeated overloading of one of the foot bones from activities such as jumping and running especially if you have suddenly increased your activity level. The breaks in the bone may be small but they can be extremely painful. Stress fractures of the metatarsal bones or the navicular can cause anything from mild to severe foot arch pain. The Tibialis Posterior muscle plays a very important role in supporting the medial arch of the foot. Posterior Tibial Tendonitis can occur either through repetitive use e.g. high impact sports such as soccer or tennis, or from an injury e.g. a fall. This causes the tendon to become inflamed or even torn, resulting in pain on bottom of foot. This pain usually gets worse with activity or when standing for long periods. If the problem persists, the inner side of the foot (known as the medial longitudinal arch of the foot) gradually collapses down, causing flat feet. A simple test for this condition is to stand on one leg and rise up onto your tiptoes. If you cannot, it indicates a problem with the Posterior Tibial tendon. Treatment usually consists of rest, ice, exercises, orthotics and physical therapy.
Symptoms
The majority of children and adults with flexible flatfeet never have symptoms. However, their toes may tend to point outward as they walk, a condition called out-toeing. A person who develops symptoms usually complains of tired, aching feet, especially after prolonged standing or walking. Symptoms of rigid flatfoot vary depending on the cause of the foot problem.
Diagnosis
A professional therapist may use tinels test to diagnose tarsal tunnel syndrome. This involves tapping the nerve just behind the medial malleolus or bony bit of the ankle with a rubber hammer. Pain indicates a positive test. Sometimes it is initially mistaken for plantar fasciitis which also causes pain from the inside heel and throughout the arch of the foot. Neural symptoms (such as tingling or numbness) as well as the location of tenderness when touching the area should help to easily distinguish between the conditions.
Non Surgical Treatment
A new ankle foot orthosis known as the Richie Brace, offered by PAL Health Systems, has proven to show significant success in treating Stage II posterior tibial dysfunction and the adult acquired flatfoot. This is a sport-style brace connected to a custom corrected foot orthotic device that fits well into most forms of lace-up footwear, including athletic shoes. The brace is light weight and far more cosmetically appealing than the traditional ankle foot orthosis previously prescribed.
Surgical Treatment
If you have pain that has not been responsive to other treatments, there is a new non-surgical treatment that was recently approved by the FDA. ESWT (extracorporeal shockwave therapy) uses strong electrohydraulic acoustic (sound) energy that triggers the body?s natural repair mechanism. This treatment method is safe, effective and requires a very short recovery period compared to older surgical techniques.
Prevention
Stretch and strengthen important muscles in your feet, ankles and legs in order to guard against future strain. Make sure to acquire suitable arch supports and inserts if necessary, and that your shoes are shock absorbent and in good condition. Wearing tattered shoes provides no protection, and runners should replace their footwear before exceeding 500 miles of usage. Athletes new to arch supports should gradually build their training routine, allowing their feet to become accustomed to a new stance.
The Causes Of Adult Aquired Flat Feet ?
Overview
Many foot problems can be contributed to Adult Acquired Flatfoot Deformity (AAFD), a foot and ankle condition that causes fallen arch of the foot. AAFD is also referred to as Posterior Tibial Tendon Dysfunction (PTTD). The posterior tibial tendon serves as the principal supporting structure of your foot. When this ligament is injured overtime the arches start to flatten, leaving you with a painful foot condition. AAFD is more common in women ages 39 - 65 than men. 
Causes
The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction. What causes adult acquired flat foot? Fracture or dislocation. Tendon laceration. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
In many cases, adult flatfoot causes no pain or problems. In others, pain may be severe. Many people experience aching pain in the heel and arch and swelling along the inner side of the foot.
Diagnosis
Observation by a skilled foot clinician and a hands-on evaluation of the foot and ankle is the most accurate diagnostic technique. Your Dallas foot doctor may have you do a walking examination (the most reliable way to check for the deformity). During walking, the affected foot appears more pronated and deformed. Your podiatrist may do muscle testing to look for strength deficiencies. During a single foot raise test, the foot doctor will ask you to rise up on the tip of your toes while keeping your unaffected foot off the ground. If your posterior tendon has been attenuated or ruptured, you will be unable to lift your heel off the floor. In less severe cases, it is possible to rise onto your toes, but your heel will not invert normally. X-rays are not always helpful as a diagnostic tool for Adult Flatfoot because both feet will generally demonstrate a deformity. MRI (magnetic resonance imaging) may show tendon injury and inflammation, but can?t always be relied on for a complete diagnosis. In most cases, a MRI is not necessary to diagnose a posterior tibial tendon injury. An ultrasound may also be used to confirm the deformity, but is usually not required for an initial diagnosis.
Non surgical Treatment
It is imperative that you seek treatment should you notice any symptoms of a falling arch or PTTD. Due to the progressive nature of this condition, your foot will have a much higher chance of staying strong and healthy with early treatment. When pain first appears, your doctor will evaluate your foot to confirm a flatfoot diagnosis and begin an appropriate treatment plan. This may involve rest, anti-inflammatory medications, shoe modifications, physical therapy, orthotics and a possible boot or brace. When treatment can be applied at the beginning, symptoms can most often be resolved without the need for surgery. 
Surgical Treatment
Many operations are available for the treatment of dysfunction of the posterior tibial tendon after a thorough program of non-operative treatment has failed. The type of operation that is selected is determined by the age, weight, and level of activity of the patient as well as the extent of the deformity. The clinical stages outlined previously are a useful guide to operative care (Table I). In general, the clinician should perform the least invasive procedure that will decrease pain and improve function. One should consider the effects of each procedure, particularly those of arthrodesis, on the function of the rest of the foot and ankle.